Fracture surgery refers to medical procedures carried out to stabilize and treat bone fractures. During the operation, cracked or broken bones are aligned or restored to their original orientation and position for proper healing. Common types of fracture surgery include open reduction and internal fixation (ORIF), and external fixation. The operation is usually performed on a person, but can also be performed on animals. [citation needed]
Fracture surgery can be performed on different bones in the human body, including hand and wrist, foot and ankle, knee, hip, femur and many more. The surgery typically involves a surgical team consisting of an orthopaedic surgeon, surgical assistants, and a nurse anaesthetist (anaesthesiologist). In internal and external fixation, metal rods, screws, plates or nails are used to provide support and secure the fractured bone until it is healed. There are certain risks for fracture surgery due to the open nature of most surgical procedures. During post-operative recovery, patients are advised to follow-up with orthopaedic surgeons or physical therapists to avoid inadequate healing, recurrent fractures, and complications.[citation needed]
The first fracture surgery was reported in France in 1775 and surgical techniques for fixation were developed at the end of the 18th century. Techniques for fracture surgery developed rapidly during the period between World War I and World War II. [citation needed]
The technique used by the orthopaedic surgeon depends on multiple criteria, including fracture location, degree of displacement, fracture pattern, and patient factors such as age and existing orthopaedic disorders. For patients with minor fractures, such as stable fracture and non-displaced oblique fracture, where the fractured bone remains at its original position, they usually do not require surgical operation and can be treated by wearing a cast.[citation needed]
In the case of severe fractures, such as compound fracture and displaced oblique fracture, where the fractured bone is visibly out of place or has pierced the skin, fixation surgical operations are typically performed to realign and stabilize the fractured bone.[citation needed] Common fixation techniques include:
Open reduction and internal fixation (ORIF) — a two-stage process...[1]. The first stage, "open reduction", involves making an incision at the site of fracture which allows orthopaedic surgeons to directly access and manipulate the fractured bone for proper alignment. The process of aligning the fractured bones is called fracture reduction. The second stage, "internal fixation", involves piercing the bone using metal implants such as rods, screws, plates, nails, or pins to hold the bone fragments in place[2]. The metal implants can be on the bone surface or inside the bone. The implants are typically harmless and left inside the body, if pain, discomfort or infection is observed, further surgery may be required to remove the implants. ORIF is preferred over closed reduction and internal fixation (CRIF) to prevent the development of post-traumatic arthrosis[3].
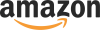
External fixation[4] — rods, screws, plates, or pins are inserted and affixed into the uninjured part of the bone. They are further connected to an external fixation device that can be adjusted to align and stabilize the fractured bone. External fixation is commonly used in scenarios with badly-damaged soft tissues to stabilize the fractured bone from a distance[5]. The fixation device may be removed once the fracture heals.File:External fixator xray.jpgExternal fixation
Other kinds of surgical procedures include:
Closed reduction percutaneous pinning (CRPP) — a minimally invasive procedure using pins to stabilize bones while minimizing soft tissue damage. Drawbacks include pin migration and less stable fixation.[citation needed]
Closed reduction and internal fixation (CRIF) — realigning the fractured bones without making incisions. A procedure called traction is carried out, where the bone is pushed or pulled to the correct position externally[6]. Internal fixation is then carried out to secure the bone in place using screws, plates, or pins.[citation needed]
Bone grafting — replacing fractured bone with transplanted bone. This procedure is used when the bone receives excessive damage and cannot be fully healed under normal fracture reduction and fixation procedures. Bone graft obtained from other bones in the body such as the hip (autograft) is used to regenerate and repair damaged areas of the bone. Sometimes bone graft from an external donor (allograft) or a synthetic source is used.[citation needed]
Treatment examples
Hand and Wrist
The vast majority of hand fractures do not require any surgical operations. However, surgery is needed for metacarpal fractures. When surgery is needed, internal fixation is the most common method. The internal fixation must be adequately strong enough to support early rehabilitation in order to prevent complications such as tendon adhesions and joint contractures.[citation needed]
Foot and Ankle
Screws are commonly used for fixation in foot and ankle fracture surgeries. Implants such as bioabsorbable pins and screws may be used.[citation needed]
Knee
In kneecap (patella) fractures, it can be repaired by internal fixation using Parallel Kirschner wires (K-wires) or using sutures[7].
Hip
The type of hip fracture surgery performed depends on the characteristics of the fracture, the age of the patient, the level of function before the injury, and the ability to participate in a postoperative rehabilitation program. Internal fixation is generally used in patients with nondisplaced or minimally displaced fractures and in patients younger than 70 years old who have displaced fractures[8]. Prosthetic replacement is performed in older patients with displaced fractures.
For an extra-articular fracture, which is a fracture that does not extend into the joint, mini-invasive surgery can be performed. All therapeutic options are also possible. For an intra-articular fracture, open reduction and internal plate fixation is normally performed for a femur fracture.[citation needed]
External fixation for femur fractures should bridge the knee when there is intra-articular involvement. In order to prevent infection, the femoral pins used should be at a distance from the fracture site and the joint[10]
Procedures
Pre-operative
Patients go through a detailed medical examination prior to the operation to determine the appropriate surgical approach. A X-ray scan of the area of injury allows the orthopaedic surgeon to assess the severity of the fracture. This is determined by the degree of displacement, fracture pattern, degree of fragmentation etc. A CT scan or MRI scan may be needed to further assess the fracture or damage in nearby soft tissues. Orthopaedic surgeons also examine the patient's health record to avoid complications due to pre-existing diseases or allergies. Once the assessment is finished, a suitable surgical approach is selected ideally to minimize damage to nearby tissues, usually CRIF for severe cases and external fixation for less severe cases. General anaesthesia (GA) or regional anaesthesia (RA) is selected depending on the scale of the surgery and the health condition of the patient, especially the elderly.[citation needed]
Intra-operative
Anaesthesia is given to the patient during the fracture surgery. An incision may be made by the surgeon over the fracture site if a plate and screws are to be used. An incision at the end of a long bone is made when a rod is placed down the interior of a bone to stabilize and repair a fracture. Metal implants such as screws, intramedullary pins (IM pins), Kirschner wires (K-wires), rods, or plates are used to secure the bone in place. These can be either temporary or permanent. Common materials for the metal implants include stainless steel and titanium alloy, which are durable, strong, biocompatible, and corrosion-resistant for long-term implantation.[citation needed]
Risks
Due to the open nature of most surgical operations, patients may risk:
To prevent infection, surgical instruments and implants are sterilized prior to the operation, antibiotics are also prescribed during preoperative and postoperative stages. Follow-up appointments with the orthopaedic surgeon are vital to monitor the progress of healing and address any concerns or complications that may arise.[citation needed]
Post-operative recovery
Patients are arranged follow-up radiographic and clinical examination to identify surgical complications or fracture recurrence, monitor fracture healing, and prescribe medication for pain alleviation. Appointments are usually scheduled once every few weeks or few months, they may extend to once every few years for long-term follow-up. Further surgery may be required if complications or long-lasting pain is observed. Patients could also see physical therapists to facilitate rehabilitation and pain management. Healing time may vary from weeks to months depending on factors such as patient health, fracture severity, and the type of surgical operation performed. For external fixation, fixation device is removed once the patient recovers. Metal implants may be removed if patients experience lasting pain or complications, but are usually left inside the body.[citation needed]
History
Before World War I
In 1775, using a wire to fix a bone was first reported in France. At the end of the 18th and in the beginning of the 19th centuries, the first techniques of operative fracture treatment were developed. Berenger-Feraud (1832-1900), a French surgeon, wrote the first book about internal fixation. However, internal fixation of fractures was uncommon until Joseph Lister, an English doctor, confirmed the safety of open reduction and internal fixation. In 1858, internal fixation using a plate and screws was first described by Carl Hansmann in Hamburg[15]
After World War I
The first techniques to perform internal fixation in the 19th century usually caused unstable fixations and carried a significant risk of infection. During the period between World War I and World War II, various plates of fixation were developed. It was also realized that a fracture of a long bone normally heals with minimal resorption at the bone ends, which might result in slight shortening and collapse. Therefore, people thought a very rigid plate might prevent such collapse. However, the use of strong plates resulted in delayed union which may also lead to insufficient stability[16]. As a result, new devices are developed so that stability can be increased.
Development of External Fixation
Malgaigne was traditionally considered to be the first to use external fixation in 1843. However, his devices were not really considered as external fixation. In 1902 Albin Lambotte invented the first "real fixator" as a device for external fixation. In America, Clayton Parkhill started the development of external fixation with a "bone clamp" in 1897. Both Parkhill and Lambotte observed the body tolerates metal pins inserted into the bone well[17]. Many external fixation devices have been and are being developed based on their research findings.

{kind=link}
{kind=link}
{kind=link}